Skeletal Muscle Relaxants
Skeletal Neuromuscular junction is one of the nicotinic receptor sites. Hence drugs can relax skeletal muscles by competitively blocking this nicotinic receptor; So, the skeletal muscle relaxants which act by this mechanism are also called competitive blockers or neuromuscular blocking agents. So this is the first important group of skeletal muscle relaxants.
- Neuromuscular blockers / Competitive blockers: Drugs including an older agent like d-tubocurarine, and newer agents like pancuronium, atracurium, vecuronium etc.
But apart from this mechanism, the skeletal muscles can be relaxed by various other mechanisms – lets list them further.
- By acting as partial agonist and then by persistent depolarization – drugs like succinylcholine
- By directly acting on the muscle fiber – like dantrolene
- And finally not by acting anywhere peripherally, but acting straight way through the central nervous system – these are called centrally acting – drugs like diazepam, chlorzoxazone, tizanidine, and baclofen
Special points
- SHORTEST ACTING NEUROMUSCULAR BLOCKER: Mivacurium
- ENDOTRACHEAL INTUBATION: Succinylcholine
- HOFFMANN ELIMINATION: Atracurium, Cisatracurium
- Succinylcholine and thiopental should not be mixed in a syringe or in an infusion. They inactivate each other. (Chemical incompatibility) (Pharmaceutical drug interaction)
- Pharmacogenetics: Succinylcholine apnea: In patients with atypical pseudocholine-esterase enzyme.
- Pharmacogenetics: Malignant Hyperthermia: In patients with abnormal Ryanodine Receptor, leading to increased calcium entry and heat production. (known with succinylcholine as well as competitive blockers)
SAQ/Viva
Classify Skeletal muscle relaxants with examples.
Skeletal muscle can be relaxed by – Peripheral Action – or by Central Action. So the drugs are divided into these 2 main types.
Among the peripheral mechanisms – 1. the drugs may competitively block the nicotinic receptor – or 2. they may act as partial agonist and persistently depolarize the muscle membrane – or 3. they may directly relax the skeletal muscle by decreasing the calcium entry.
The centrally acting drugs include GABA-A agonists, Mephenesin group, GABA-B agonists, and Central Alpha-2 agonists (Tizanidine).
(A) PERIPHERALLY ACTING
- Competitive blockers/Neuromuscular blokcrs: d-tubocurarine, pancuronium, atracurium, mivacurium, rocuronium
- Partial agonist/Persistent Depolarizing agents: Succinylcholine
- Directly acting: Dantrolene
(B) CENTRALLY ACTING
- GABA-A agonists: (Benzodiazepines): Diazepam
- Mephenesin group: Chlorzoxazone
- GABA-B agonist: Baclofen
- Central Alpha-2 agonist: Tizanidine
Competitive blocking agents or Neuromuscular blocking agents are further classificd as follows:
A. LONG ACTING: Pancuronium (newer), D-tubocurarine (=Curarine) (=Curare) (Older agent)
B. INTERMEDIATE ACTING: Atracurium, Cisatracurium (Hoffmann elimination), Vecuronium, Rocuronium
C. SHORT ACTING: Mivacurium (shortest acting)
SAQ/Viva
Explain mechanism of action of succinylcholine.
(While answering this question, please avoid discussion of what is the mechanism of action of succinylcholine in various species such as rats, frogs, monkeys etc….this will avoid unnecessary confusion)
Succinylcholine is a partial agonist which combines with the nicotinic receptor to produce depolarization and a feeble contraction. It dissociates slowly from the receptor, hence it leads to persistent depolarization.
Succinylcholine acts as a partial agonist at nicotinic cholinergic receptor.(Partial agonist has equal affinity for the receptor, but the intrinsic activity is less than that of the agonist). So it combines with receptor and produces depolarization; but the intrinsic activity is less. (This can be observed as feeble contractions of the muscle in the form of twitching and fasciculations). [Because this is the phase of depolarization, sometimes it is called as Phase I block or depolarization block].
Succiuylcholine does not get dissociated from the receptor immediately. Hence the muscle memtrane remains in persistent depolarization, and hence it remains insensitive to any further stimuli. Thus the skeletal muscle remains relaxed. [During this period, the muscle end plate is desensitized to further stimuli, hence this phase is sometimes called phase 2 block or desensitization block].
This is the mechanism of action by which succinylcholine produces skeletal muscle relaxation.
SAQ/Viva
Mention the conditions in which succimylcholine is used.
Succinylcholine is a skeletal muscle relaxant acting by persistent depolarizing agent. It is short acting and extremely useful for procedures of short duration as well as endotracheal intubation.
Uses:
- Endotracheal intubation (For passing tracheal tube) required during anesthesia and other situations
- Short procedures e.g. Laryngoscopy, bronchoscopy, esophagoscopy.
- For reduction of fractures and dislocations
- For treating acute laryngospasm
- To prevent convulsions and trauma from electroconvulsive therapy (ECT).
SAQ/Viva
Mention adverse effects of succinylcholine.
Succinylcholine is a skeletal muscle relaxant acting by persistent depolarization. It is a partial agonist of acetylcholine.
Adverse effects:
- Hyperkalemia: Due to increased potassium release from intracellular stores.
- Post-operative muscle soreness (muscle pain) due to release of potassium
- Cardiac arrhythmia due to hyperkalemia
- Malignant hyperthermia This genetic condition (autosomal dominant) is shown in susceptible individuals [having abnormal Ryanodine receptor (RyR)]. It is precipitated in presence of succinylcholine as well as volatile general anesthetics (ether/halothane/isofluraine/enflurane/sevoflurane etc). There occurs increased calcium entry in the skeletal muscle – leading to increased muscle tone, rigidity, increased heat production and severe increase in body temperature, myoglobinuria, metabolic acidosis, and in severe cases multiple organ failure. Treatment of malignant hyperthermia is – external cooling, antipyretic drugs, intravenous fluids, intravenous sodium bicarbonate, and a directly acting muscle relaxant such as Dantrolene (which decreases the calcium entry and decreases heat production).
- Succinylcholine apnea: This genetic condition (autosomal recessive) is precipitated in patients having atypical pseudocholine-esterase enzyme. (In individuals in whom this enzyme is normal, it is supposed to break down succinylcholine). The patients in whom pseudocholine-esterase enzyme is atypical, succinylcholine does not break down and it accumulates, and leads to prolonged muscle relaxation, leading to paralysis of diaphragm and intercostal muscles, leading to apnea. Treatment of succinylcholine apnea is – Fresh blood transfusion (which will supply pseudocholinesterase enzyme from the blood to break down succinylcholine) and artificial respiration.
SAQ/Viva
Mention mechanism of action and uses of Dantrolene.
Dantrolene is a DIRECTLY ACTING SKELETAL MUSCLE RELAXANT.
It binds to the Ryanodine receptor (RyR) on the sarcoplasmic reticulum and blocks their opening, and prevents Calcium release from sarcoplasmic stores.
Uses:
- To reduce spasticity in conditions such as upper motor neurone disorders, hemiplegia, paraplegia, cerebral palsy, multiple sclerosis – by oral route of administration.
- In management of malignant hyperthermia – it helps to decrease the heat production and muscle rigidity by blocking calcium release from sarcoplasmic reticulum – useful by intravenous route.
LAQ/SAQ/Viva
Compare and contrast: d-tubocurarine and succinylcholine (same question may be framed as Competitive blockers and Depolarizing agents)
See below the answer in table form. It is made with an objective to cover all aspects of the two drugs. Most important points are mentioned earlier; so remember in the same sequence.
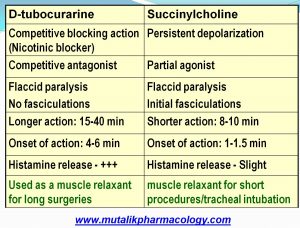
The first table compares their mechanism, onset and duration of action, and the way the drugs are used. D-tubocurarine is a competitive nicotinic blocker with slower onset and long duration of action, so it is preferred for major or longer surgeries, whereas succinylcholine is a partial agonist with persistent depolarizing action, and has rapid onset and short duration of action, so is naturally preferred for short procedures and for tracheal intubation. With this understanding, read the table below:
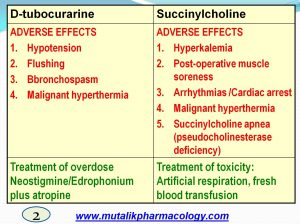
The next table describes the adverse effects and treatment of toxicity/overdose. D-tubocurarine like drugs release histamine and hence are likely to produce vasodilation and flushing, bronchospasm, and hypotension; and these are less likely with succinylcholine as histamine release is minimal with succinylcholine. On the other hand, succinylcholine is known to produce hyperkalemia, and hence produces post-operative muscle soreness and has chances of producing cardiac arrest or arrhythmias. So also it precipitates apnea in individuals with pseudocholinesterase deficiency. Both d-tubocurarine and succinylcholine have chances of producing malignant hyperthermia in susceptible individuals.
D-tubocurarine is a nicotinic blocker, so its overdose is treated with anticholinesterase drugs (neostigmine / edrophonium) that will potentiate acetylcholine. On the other hand succinylcholine toxicity is treated with fresh blood transfusion to supply cholinesterase enzyme to destroy the accumulated succinylcholine, and artificial respiration to help overcome the apnea. Understand these facts in the table below.
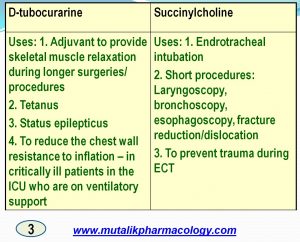
Next, we go on the describe the detailed uses of the two groups/drugs. Read in the table below:
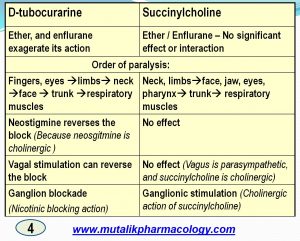
If you are interested in more complex details, go to the last table below:
SAQ/Viva
Mention centrally acting skeletal muscle relaxants and their uses pertaining to muscle relaxation.
Centrally acting skeletal muscle relaxants include:
a. GABA-A agonists: Benzodiazepines: Diazepam
b. Mephenesin group: Chlorzoxazone
c. GABA-B agonists: Baclofen
d. Central Alpha-2 agonists: Tizanidine
Diazepam is useful in most of the conditions mentioned below. Baclofen is also useful in intractable hiccups and also in most of the following conditions (except cerebral palsy). Tizanidine is useful in muscle spasms and conditions related to spinal cord injury and multiple sclerosis. Chlorzoxazone is mostly useful in conditions mainly related to peripheral musculoskeletal system.
Uses:
1. Acute muscle spasms; overstretching, sprain, tearing of ligaments-tendons, dislocations, bursitis, rheumatic disorders
2. Torticollis, lumbago, backache, neuralgias (trigeminal neuralgia)
3. Hemiplegia, paraplegia, spinal injuries, tardive dyskinesia, multiple sclerosis, cerebral palsy
4. Intractable hiccups: Baclofen
5. Tetanus
6. Status epilepticus
7. Spasticity, Amyotropic laternal sclerosis, spinal injuries
SAQ/Viva
What is Hoffmann elimination? What is its importance for skeletal muscle relaxants?
Hoffmann elimination means Spontaneous molecular rearrangement leading to breakdown and inactivation of certain drugs without any enzyme. The exact mechanism behind this phenomenon is not known.
Amongst the skeletal muscle relaxants, Atracurium, Cisatracurium undergo Hoffmann elimination.
If a patient suffers from hepatic failure or renal failure, most of the skeletal muscle relaxants would not be metabolized or excreted to sufficient extent, and hence would accumulate in the body and lead to toxicity.
In such situations, atracurium or cisatracurium prove to be beneficial, because they don’t need to be metabolized by liver. They undergo Hoffmann elimination (spontaneous degradation and elimination). This is the importance of Hoffmann elimination.
So also in neonates and in very old patients, the liver function and the renal function may be low. Hence in these patients also, atracurium and cisatracurium are especially beneficial.
SAQ,Viva
Thanks for pointing out the error. Accordingly the correction is made. Sorry for the inconvenience.