Adrenergic Agonists
Autonomic Nervous System (ANS) Receptors mostly follow a certain predictable behavior. If we understand this, ANS is one of the most interesting topics in Pharmacology.
SAQ/Viva
What is the general rule about actions of adrenergic receptors? Mention the exceptions.
Below is a chart to explain the normal/general rule and exceptions. Now read the following matter along with the chart loudly, and referring to the chart in between, as if you are reading out from the chart.
Upward arrow means Stimulation / Excitation.
Downward arrow means Depression / Inhibiton.
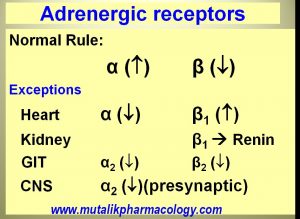
The normal rule for adrenergic receptors is –
Alpha receptors are stimulant/excitatory.
Beta receptors are inhibitory/depressant.
The exceptions to this rule are:
- Heart : Exactly opposite. Alpha depressant and Beta stimulant. And the Beta in heart are Beta-1. The stimulation of these Beta-1 will lead to increased force and rate of contraction of the heart and increased cardiac output and oxygen consumption. For practical purpose, the number of alpha receptors in heart can be considered negligible..
- Second exception is Kidneys. Here also the Beta are stimulant and they are Beta-1 and they stimulate the Renin secretion.
- GIT: in GIT, both Alpha and Beta are depressant, and they are Alpha-2 and Beta-2.
- In the CNS, there are Alpha-2 receptors which are pre-synaptic, and they are inhibitory in nature. Stimulation of these receptors leads to Decreased sympathetic outflow to the periphery. Stimulation of these receptors by drugs like clonidine or methyldopa leads to decrease in blood pressure, because the receptor is inhibitory in nature.
SAQ/Viva
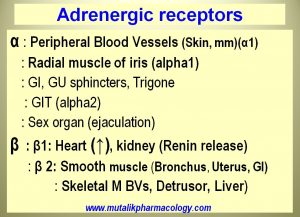
Mention the sites for adrenergic receptors.
The following charts shows important alpha and beta receptor sites of adrenergic receptors. Read them with the description given above about the general rule and exceptions, so that you will understand what action happens.
SAQ/Viva
Mention important alpha receptor sites and the actions that take place on stimulation of alpha receptors.
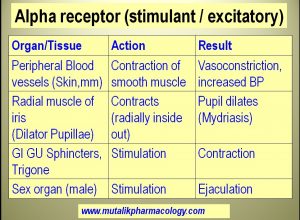
1. Alpha receptors in the peripheral blood vessels are stimulant and their stimulation by adrenergic agonists will produce contraction of the smooth muscle of these blood vessels, leading to vasoconstriction and increase in blood pressure.
Implications:
- Adrenaline (epinephrine), noradrenaline, dopamine, and more selective agonists like methoxamine, metaraminol, mephenteramine, and phenylephrine shall stimulate this receptor to produce vasoconstriction and will increase the blood pressure, and hence are useful in shock.
- Ephedrine, pseudoephedrine, xylometazoline, oxymetazoline, naphazoline, phenylephrine, when used as nasal drops will stimulate the alpha receptor to produce vasoconstriction, and thus will be useful as nasal decongestants. (Vosodilation = Congestion; vasoconstriction = decongestion).
- Epinephrine stimulates the alpha receptors to produce vasoconstriction, so when used with lidocaine (a local anesthetic), leads to decreased local blood flow, decreased rate of entry of local anesthetic into systemic circulation. So it is slowly removed from the local tissue. Thus its contact time with the nerve fiber is increased; leading to prolongation of duration of action of local anesthesia.
- Epinephrine (adrenaline) stimulates alpha receptors to produce vasoconstriction and increase in blood pressure, hence useful in anaphylactic shock to treat hypotension.
2. Phenylephrine and ephedrine like drugs shall stimulate the alpha receptor to produce contraction of radial muscle of iris, to produce dilation of pupil (mydriasis)
SAQ/Viva
Mention important beta receptor sites and the actions that take place on stimulation of alpha receptors.
Beta-1 receptors
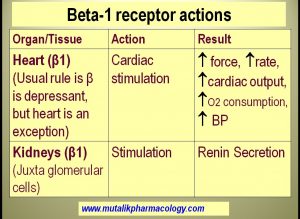
For practical purposes, Remember 2 important Beta-1 sites.
- Heart: By normal rule Beta receptor is supposed to be inhibitory, but heart is an exception, and the Beta -1 receptor in the heart is stimulant. So its stimulation by adrenergic agonists (adrenaline, isoprenaline) leads to increased force and rate of contraction, increased cardiac output and blood pressure, and increased myocardial oxygen consumption. Therefore drugs like adrenaline or isoprenaline can be used to treat cardiac arrest to resuscitate the heart. Similarly, beta blockers (atenolol, metoprolol, propranolol) shall block the beta receptors and decrease the heart rate and blood pressure.
- Kidneys: Beta-1 receptor in the juxta-glomerular cells is stimulant in nature, and hence leads to renin release. So adrenergic agonists produce increase in blood pressure. Decrease in plasma renin activity is one of the mechanisms of beta blockers in decreasing the blood pressure.
Beta-2 receptors
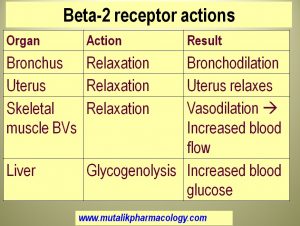
- Bronchus: Beta-2 receptor in bronchial smooth muscle is inhibitory in nature. So its stimulation leads to bronchodilation (relaxation of bronchial smooth muscle). Adrenergic agonists (adrenaline, ephedrine, isoprenaline) and selective adrenergic agonists (salbutamol, terbutaline, salmeterol, formoterol) produce brochodilation and thus are useful to relieve the brochospasm e.g in bronchial asthma). Beta blockers (propranolol-like drugs) block this receptor, and hence bronchospasm is one of the known adverse effects of beta blockers. Hence they are contraindicated in patients with bronchial asthma.
- Uterus: Similarly Beta-2 receptor associated with uterine muscle is also inhibitory. So its stimulation leads to uterine relaxation. Adrenergic agonists like Isoxsuprine, Nylidrine, Ritodrine selectively stimulate this receptor and act as “Uterine Relaxants”. Hence they are useful in management of Premature labor, Dysmenorrhea, and Threatened abortion. (Tokos = childbirth. Lytic= Oppose, prevent). They prevent the contraction of uterus and keep it relaxed.
- Skeletal muscle blood vessels: contain Beta-2 receptor which when stimulated by adrenergic agonists, leads to vasodilation of blood vessels supplying the skeletal muscles, so that the blood flow to skeletal muscles is increased.
- Liver: Beta-2 receptor in liver is responsible for breakdown of glycogen and increasing the blood glucose. This is why sympathetic nervous system helps us in events of hypoglycemia. Adrenergic agonists help in the same way.If a patient is taking non-selective beta blockers like propranolol, then there is blockade of these Beta-2 receptors. If this patient goes into hypoglycemia, then because the beta-2 receptors is blocked, there is no correction of hypoglycemia and no response to hypoglycemia (Beta-1 in heart are also blocked by beta blockers). This is called hypoglycemia unresponsiveness. This is especially likely in patients prone to hypoglycemia (patients with diabetes mellitus). Hence Beta blockers are generally avoided in patients with diabetes mellitus.
SAQ/Viva
Compare and Contrast: Catecholamines and Non-catecholamines.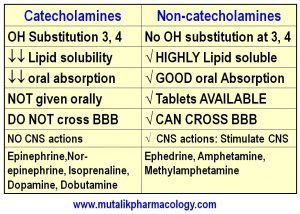
SAQ/Viva
Mention Pharmacological actions of Adrenaline (Epinephrine).
Adrenaline is an adrenergic agonist. It stimulates Alpha as well as Beta receptors.
Pharmacological actions:
1. Stimulates the heart: (Beta-1 receptors)
Increases –
- Contractility (ionotropic), Rate (Chronotropic), Conductivity (Dromotropic), Excitability (Bathmotropic)
- Force of contraction
- Heart rate
- Cardiac output
- Myocardial oxygen consumption, and
- Systolic blood pressure
2. Dilates the bronchus: Brochodilation: (Stimulates Beta-2 receptor):
- Activates adenylyl cyclase (=adenylate or adenyl cyclase)
- Adenylyl cyclase catalyzes conversion of ATP to cAMP.
- cAMP dependent protein kinase A (PKA) is activated.
- So, Myosin Light Chain Kinase (MLCK) is phosphorylated to its inactive form, so that the smooth muscle contraction is prevented.
- So, Bronchial smooth muscle relaxation. (Bronchodilation)
3. Vasoconstriction (Smaller blood vessels): Stimulates Alpha-1 receptors: Important for clinical application: Nasal blood vessels, Blood vessels around the teeth
4. Physiological Antagonist of Histamine: Opposes actions of Histamine.
- (Histamine – vasodilation , Adrenaline – Vasoconstriction)
- (Histamine – Hypotension, Adrenaline – Increases blood pressure)
- (Histamine – Bronchospasm, Adrenaline – Bronchodilation).
5. Increases blood sugar:
- Stimulates Beta-2 receptor -Glycogenolysis
- Stimulates Alpha receptor – Inhibits insulin release
- Increases glucagon release
SAQ/Viva
Mention therapeutic uses of Adrenaline (Epinephrine). Mention the basis for each use.
Adrenaline is an adrenergic agonist that stimulates Alpha as well as Beta receptors.
Its therapeutic uses depend mainly on the vasoconstriction in smaller blood vessels (Alpha-1), stimulation of heart (Beta-1), and dilation of bronchial smooth muscle (Beta-2).
- Uaed along with local anesthetic (e.g. lidocaine) to prolong the duration of action of local anesthesia. This is the most common use of adrenaline. (1:100,000 or 1:200,000 of adrenaline). (Mostly 1:200,000 in dental anesthesia) is preformed with lidocaine for infiltration as well as nerve block anesthesia for tooth extracction). [Basis: – Adrenaline produces vasoconstriction by stimulating alpha receptors in the smaller blood vessels -Decreases the rate of entry of the local anesthetic into systemic circulation — and thereby decreases the rate of its removal from local tissue —thus increases its contact time with the nerve fiber —–and thus prolongs its duration of action. Because the systemic absorption of local anesthetic is minimized, the chances of its systemic toxicity are reduced.] [Additionally, bleeding is minimized]
- Used to stop minor bleeding (bleeding from smaller blood vessels): By local application of adrenaline pack for “Epistaxis” ( nasal bleeding) or by injecting with local anesthetic or as a local pack for bleeding after tooth extraction. (1:10,000 or 1:200,000 of adrenaline). [Basis: Adrenaline – stimulates Alpha receptor, constricts the smaller blood vessels, and controls bleeding].
- Acute Anaphylactic Shock: Adrenaline relieves brochospasm, stimulates the heart to maintain cardiac output, and constricts smaller blood vessels, and maintains the blood pressure. Reverses the manifestations of histamine release including breathlessness, hypotension, itching, and skin rashes. [Basis: This is the type I – Immediate hypersensitivity reaction. Adrenaline stimulates Beta-1 receptor in heart to increase contractility and cardiac output, stimulates Alpha-1 receptor to produces vasoconstriction and increases systolic blood pressure, and stimulates Beta-2 receptor of bronchial smooth muscle to relieve bronchospasm. Physiological antagonist of histamine, reverses histamine actions of breathlessness, hypotension, myocardial suppression, and skin rashes and itching].
- Acute attack of bronchial asthma: Relieves bronchospasm when used by subcutaneous or inhalation. Not commonly used. [Basis: Stimulates Beta-2 receptor, dilates the bronchus].
- For cardiac resuscitation in a case of cardiac arrest: In cardiac arrest due to electric shock or drowning. [Basis: Stimulates Beta-1 receptor in heart to resuscitate it].
SAQ/Viva
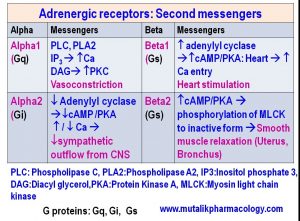
Mention the second messengers in adrenergic receptors with the implications.
Adrenergic receptors are G-protein coupled receptors, with 3 important G proteins, namely, Gq, Gs, and Gi. The messengers for the most important receptors are as follows:
SAQ/Viva
Classify adrenergic agonists with examples.
Simplest and most useful way to classify is as follows:
- NON-SELECTIVE ADRENERGIC AGONISTS: These act on Alpha as well as Beta receptors without much selectivity for any receptor types.
(a) Catecholamines: Adrenaline, Nor-adrenaline, Isoprenaline, Dopamine, Dobutamine
(b) Non-catecholamines: Ephedrine, Amphetamine, Methyl-amphetamine, Methyl phenidate
2. SELECTIVE ADRENERGIC AGONISTS: They have selectivity for certain receptors and certain sites, hence they are useful in specific conditions, and also shall have minimal unwanted effects on other sites..
(a) BRONCHODILATORS: Bronchial asthma (Selective B2 agonists):
SHORT ACTING: Salbutamol (Albuterol), Levsalbutamol, Terbutaline, Metaproterenol (Orciprenaline), Pirbutarol
Salbutamol inhaler device

LONG ACTING: Salmeterol, Formoterol
(b) UTERINE RELAXANTS: (TOCOLYTICS): (Selective B2 agonists) USES:Threatened abortion, dysmenorrhea, premature labor
Examples: Isoxsuprine, Nylidrine, Ritodrine
(c) NASAL DECONGESTANTS: (alpha agonists) (produce vasoconstriction in nasal blood vessels) [congestion = vasodilation, decongestion = vasoconstriction]
Examples: Pseudoephedrine, xylometazoline, oxymetazoline, naphazoline, phenylephrine
(d) VASOPRESSOR AMINES: (alpha agonists): (alpha agonists: Constrict peripheral blood vessels and increase the blood pressure): Used Intravenously for Hypotensive Shock.
Examples: Methoxamine, metaraminol, mephenteramine, Phenylephrine
(e) MYDRIATICS: (Alpha agonists): (alpha agonists: contract the radial muscle of iris, decrease intraocular pressure): Used locally in eye:Phenylephrine (to dilate the pupil – active mydriasis), Dipivefrine ( a prodrug of epinephrine for treatment of glaucoma), Apraclonidine, Brimonidine (Glaucoma)
(f) ANOREXIANTS: (Act on CNS, Decrease apetite): Fenfluramine
(g) CENTRAL ALPHA-2 AGONISTS: (Decrease the sympathetic outflow from CNS and decrease blood pressure): Clonidine, Methyldopa
SAQ/LAQ/Viva
Explain the rationale (basis), advantages, and contraindications for lidocaine-epinephrine combination.
Epinephrine prolongs the duration of action of local anesthetic.
Lidocaine is a local anesthetic of amide group. It is often combined with vasoconstrictors like Epinephrine (adrenaline) (1:50,000 or 1:100,00 or 1:200,00), levonordefrine (1:200,00) or phenylephrine (1: 20,000)
Combining adrenaline with local anesthetic produces following effects and advantages:
- Adrenaline produces vasoconstriction in the small blood vessels (Stimulates Alpha-1 receptors)
- Decreases the rate of entry of local anesthetic into systemic circulation
- Decreases the rate of removal of local anesthetic from the local site
- More contact time of local anesthetic with nerve fiber.
- Prolonged duration of action of the LA
The advantages are:
- Duration of action of anesthesia (60-120 minutes) may be increased upto 2.5 to 3 hours.
- Systemic absorption of local anesthetic is miniminzed.
- Systemic adverse effects of local anesthetic are minimized. (Reduced systemic toxicity of local anesthetic)
- Bleeding is minimized due to vasoconstriction
- Need for additional analgesics is minimized.
Contraindications:
- Sites supplied with end arteries where ring block anesthesia may be given (fingertips, toe-tips, male sex organ, some areas in ear/nose/throat region), where lack of blood supply may lead to ishemia and necrotic changes
- Severe hypertension
- Severe Cardiac Arrhythmias
- Severe cardiac disease including recent history of Angina/Myocardial infarction/Heart failure
Disadvantages:
- Some chances of delayed wound healing
- Possibility of tissue hypoxia
- Likelihood of necrosis/tissue edema
SAQ/LAQ/Viva